



Australia’s asthma hotspots have been revealed in a new UNSW Sydney-led study, which found higher proportions of childhood asthma in areas with greater disadvantage and a higher Indigenous population.
Asthma is more common among children in regional Australia, occurring at more than double the national average in some communities, new research shows.
The nation’s asthma hotspots are largely found in regional and rural communities with greater socioeconomic disadvantage and higher proportions of Indigenous Australians, the study led by UNSW Sydney shows.
The study, published in Global Health Research and Policy, found hundreds of childhood asthma hotspots across the country, the bulk of which were in regional or remote areas of New South Wales, Victoria, Queensland, and Tasmania.
Lead author Dr Jahid Khan, from UNSW’s School of Clinical Medicine, said a link between asthma and social deprivation had been expected, as with many chronic conditions, but that the scale of the difference across communities was greater than anticipated.
“We suspected there would be an elevated proportion of children with asthma in areas of greater deprivation, but to see such a difference within one country and so many areas of hotspots, it surprised us,” Dr Khan said.
“This highlights to policymakers the areas where more resources and more targeted intervention are needed, to reduce the burden of asthma among children, as well as the associated hospital costs and health expenditure.”
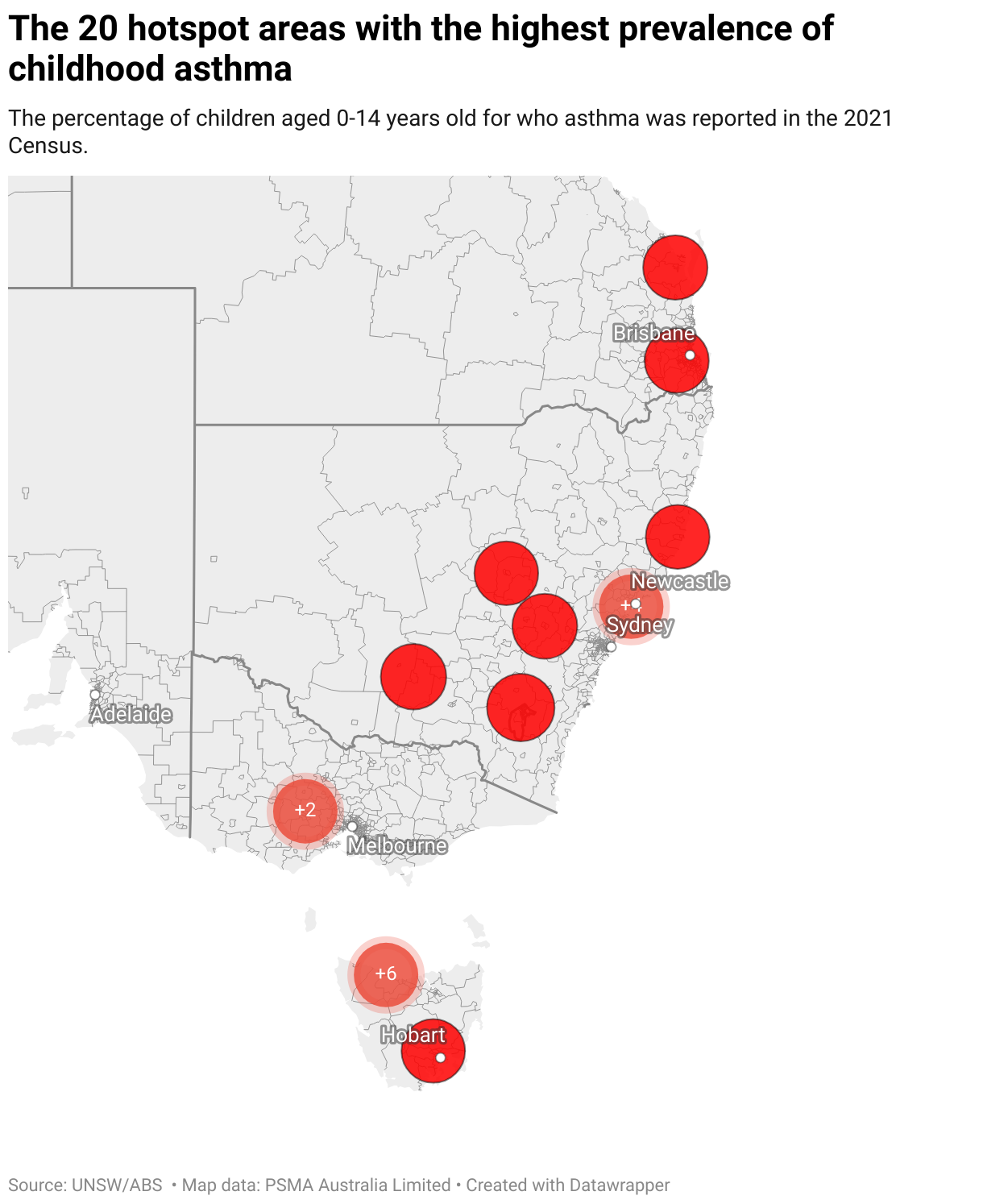
Australia's childhood asthma hotspots
UNSW researchers collaborated with asthma experts from across the country including the Sydney Children’s Hospitals Network, Murdoch Children’s Research Institute and The Royal Children’s Hospital Melbourne.
They analysed asthma prevalence in children and teenagers, up to age 14, and sociodemographic features, in 2321 communities, using Statistical Areas Level 2 (SA2) data from the 2021 Census – the first to collect information on diagnosed long-term health conditions.
Of those, 465 or 20%, were part of an asthma hotspot. An area was deemed a hotspot when there was a cluster of communities with an above average prevalence of childhood asthma.
Media enquiries
For enquiries about this story and interview requests, please contact Kate Burke, News & Content Coordinator, UNSW Medicine & Health.
Tel: +61 2 9348 2538
Email: kate.burke@unsw.edu.au


The proportion of children with asthma in identified hotspots reached as high as 13.8% in the Action-Upper Burnie region on Tasmania’s north coast, more than double the national average of 6.27% for children, which was recorded across the analysed regions.
It was followed by Tasmania’s East Devonport region (12.8%) and the Mount Hutton – Windale region (12.9%), in NSW’s Lake Macquarie.
Hotpots were also found in the Central Coast, Riverina and New England regions in NSW, Shepparton, Ballarat and Bendigo in Victoria, Ipswich and Logan in Queensland.
More than 60% of hotspots were in socioeconomically disadvantaged areas and another 21% were in areas of medium disadvantage. The proportion of Indigenous people was also elevated – above the national SA2 median of 2.08% – in more than 80% of hotspots.
Overall, childhood asthma prevalence ranged from 0 to 16.5%, but some areas with the highest proportions were outliers, which did not fall in hotspot clusters.
Factors that can contribute to asthma
Environmental factors, socioeconomic deprivation, ethnicity and limited access to health care could all be contributing to the trend, said senior report author Dr Nusrat Homaira, a senior lecturer with UNSW’s School of Clinical Medicine.
“People on lower incomes are more likely to be in substandard housing, where there can be greater exposure to triggers like mould and dust mites or may be living in areas where there are higher levels of air pollution or pollens.”
Respiratory infections, which are more common in overcrowded housing due to the higher risk of spreading infections, were also a key asthma trigger, Dr Homaira said.
On top of these triggers, those in regional and remote communities have greater difficulty accessing appropriate health care, as most specialist paediatric asthma services were based in metropolitan hospitals, Dr Homaira added.
“They have limited access to healthcare resources, which results in poor asthma control,” she said.
More support needed in regional Australia

The healthcare barriers faced in regional communities are all too familiar for Ebony Elliott and her 10-year-old daughter Oakley Elliott, who has a rare form of complex asthma.
Oakley, a Year 4 student, and her parents routinely make the 1100-kilometre round trip from their home in the Albury region to the Sydney Children's Hospital Randwick, where Oakley receives treatment at the Complex Asthma Clinic.
They’re incredibly grateful for the care she receives there but wish there could be more treatment options and specialist support closer to home.
“Oakley has had 10 weeks off sick from school already this year. The fact that we need to travel away to get treatment, that is adding to that time we already know she is going to have off, that is another stress for her and our family,” said Ms Elliott.
On top of the distance and time, there is also the cost and juggling act, as Oakley’s parents must take time off work to travel to Sydney, while also caring for their three other children. Without charities like Ronald McDonald House and Little Wings, which provide support for families in need of accommodation and flights, the trips would not be achievable, she noted.

Even getting a diagnosis for Oakley’s asthma proved a challenge in her hometown. It took many months and persistence from the family, before eventually being referred to specialists in Sydney after multiple trips to the ICU.
“Oakley would get a cold and end up in the ICU and we weren’t quite sure what was going on. We saw a few doctors and they told us she didn’t have asthma ... eventually a doctor there advised us to get a second opinion,” Ms Elliott said.
“Oakley's life is much better since getting her diagnosis and the right treatment. I would still say she has the same amount of hospital admissions, but she hasn’t been as seriously ill.
“I often think about what if I had just accepted when they said everything was fine, what if I just left it. There would be many people that don’t have the knowledge and experience to know it’s not fine, that they do need more help and that’s the scary thought for me.”
News that their community has an above average rate of childhood asthma, at 7.7%, is little surprise to the family, who know of a lot of children with asthma in the area – some of whom must also travel for treatment.
While local pediatricians have developed relationships with Oakley’s specialists in Sydney, it would be amazing to see more specialist support in regional Australia, Ms Elliott said. Easier access to medication would also be key, as some were only available in Sydney.

Where to next?
Researchers hope the study will pave the way for better targeted resourcing and intervention for asthma treatment and management.
“That might look like making sure we have a community nurse in place who can liaise with these children and make sure that they get the care that they need and that their parents or carers are given the asthma education that they need,” Dr Homaira said.
However, they noted further investigation was still needed to drill down into the key driving factors at play across the identified hotspots, so government and policymakers could better address health inequity.
“We know that in Australia almost 40% of all health outcomes in children can be explained by socioeconomic disadvantages. Even in a country like Australia, there's significant disparities that determine a child's health trajectory over the years,” Dr Homaira said.
“While there are unchangeable factors like genetics or birthplace, there are aspects of a child’s environment that can be influenced. Addressing socioeconomic disadvantages is one of the most significant ways Australia can improve children’s health outcomes,” she said.
Related stories
-

Children with asthma not at higher risk of severe COVID, research suggests
-

New asthma medicine restrictions will hurt the poorest children the most
-

Kids hospitalised with chronic illness up to three times more likely to fall behind at school
-

How to protect yourself against bushfire smoke this summer